

Tuesday 24th March 2020

A short history of epidemics
Like a well orchestrated theatrical play history shows us that epidemics are structured into three acts:
(1) Act I- Society acts for self-reassurance and acts to protect the economy. The impacts on society are subtle and life appears relatively normal. The first act begins its conclusion as morbidity and mortality from the disease accelerates sharply. There is acceptance by expert communities for the need of more stringent methods of disease containment. This act started as an uplifting tale, full of defiance in the face of adversity, however it rapidly descends into darkness as the true nature and scale of the issue dawns.
(II) Act II- This act begins with more widespread recognition of the issues amongst the population. Analysis of the problem at hand and explanation delivered to society. Virtue determines the length and course of this act- hysteria and panic leads to social unrest whereas co-ordinated moves by government and morals in society smooth the journey and lead to a succinct conclusion.
(III) Act III- The final act: resolution. The action of government and society affect the spread of the epidemic. Widespread vigilance is maintained to reduce incidence of further spread. A lingering tone of unease is left in society. Fin. (1)

There is desire from scientific communities to identify the source of infections. Our latest thesis is the current pandemic due to SARS-CoV 2 virus was transmitted to humans from pangolins, armadillo-like animals, known carriers of coronaviruses. The virus is closely related to two bat derived severe acute respiratory distress syndrome-like coronaviruses. (2) Some experts are discussing the possibility of multiple interspecies transmissions. However, what we know so far it that the SARS-CoV 2 likely did not originate in humans and required at least one interspecies jump to infect homo sapiens.
The first incidents of COVID-19 caused by the SARS-CoV 2 virus were cases of atypical pneumonia in Huanan Seafood Market in Wuhan, China. Understanding the origins of epidemics allows for epidemiological study and contact tracing however it does open the possibility for prejudice towards certain groups in society.
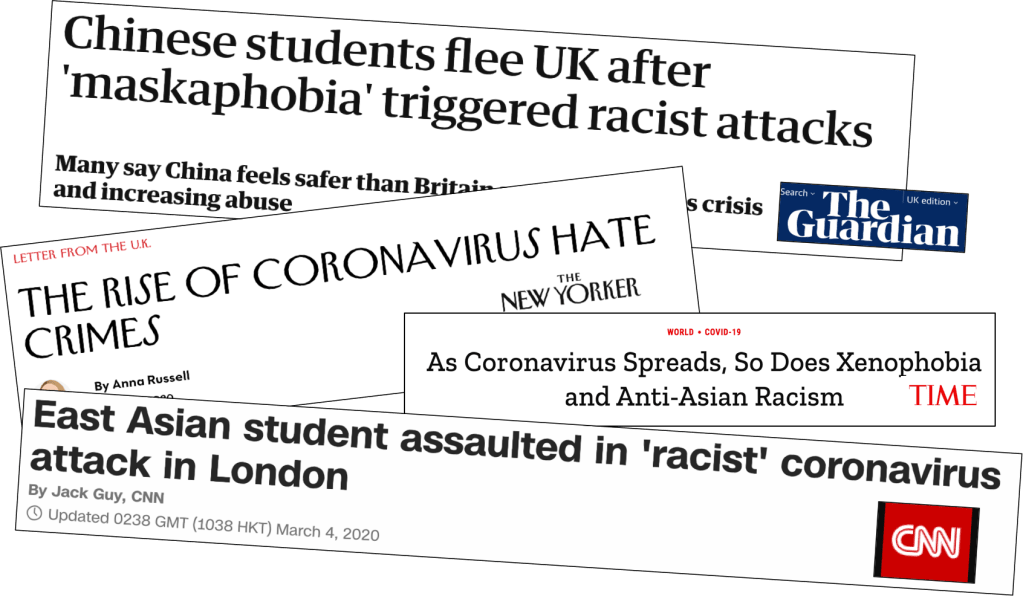
In recent years, there has been a shift towards right-wing, nationalistic ideology in much of Europe and the United States of America. Exemplified by Brexit, anti-EU agendas, the US-China trade war and Donald Trump’s anti-immigration policies. China has been viewed as a rising economic and industrial superpower, a pseudo-democracy that threatens the status quo of western economic and political dominance. How will the rise of the COVID-19 global pandemic, originating in China, during a period of anti-immigrant rhetoric influence societal views on China and it’s people? Will this lead to greater nationalism and further stigmatisation of foreigners in our society? The evidence suggests so with several racially-motivated assaults on those from East Asian background within the UK in the past several weeks.
What else can history tell us about epidemics? Fears can be exaggerated and cause mass panic amongst the general public. Whilst the death toll from the SARS-CoV 2 virus has been substantial and deeply saddening to put this pandemic into perspective, today is World TB day, which profiles a disease that is estimated to infect up to one-third of the global population and kills 4000 people a day. Half a million people a year die from seasonal influenza and road traffic accidents kill 3500 people a day according to the World Health Organization. (3) Scientific collaboration and government action, not widespread panic, is required now to reduce the disease burden and thankfully this is what is being seen.
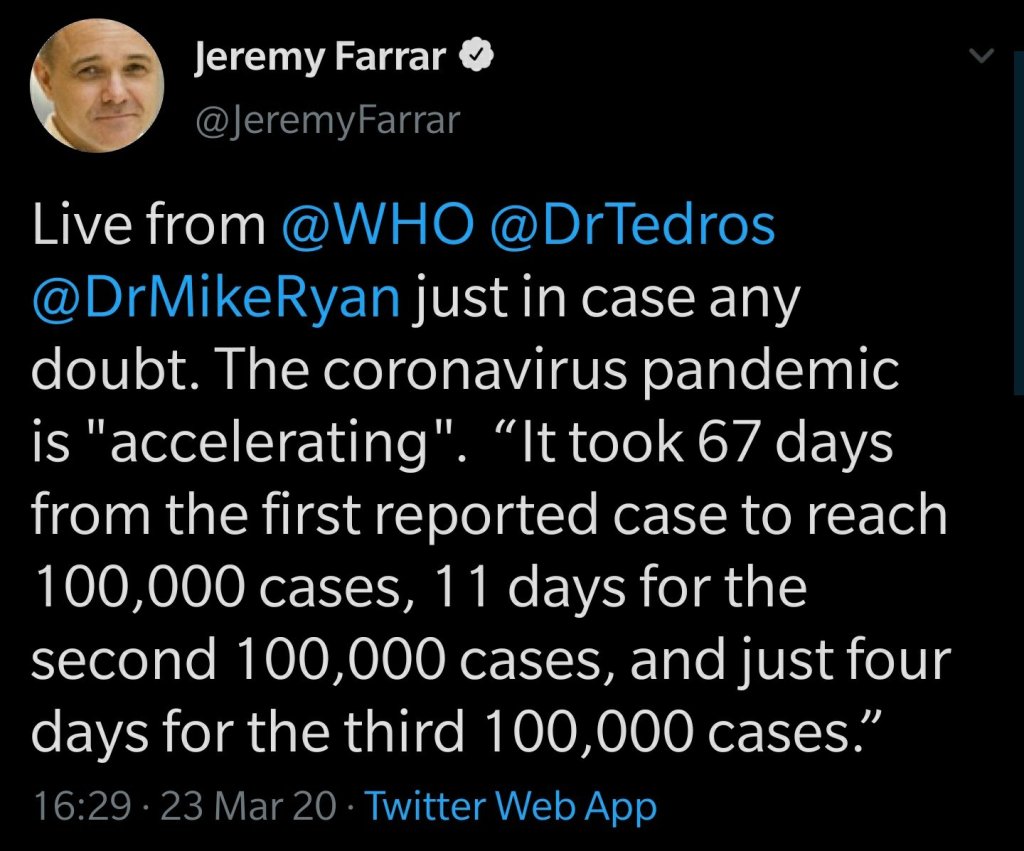
However COVID-19 has the potential to spread rapidly across the world and cause significant socioeconomic damage, perspective should be maintained at this time to prevent widespread panicked behaviours. We must have faith in our scientific community and government to direct us to behave appropriately and keep Act II of this play as short and smooth as possible.
Basic Epidemiology
SARS-CoV 2 is ‘transmitted’ or spread by aerosolised respiratory droplets or via direct contact. Current theories suggest that the virus remains stable on a number of different surfaces. The virus was detectable on plastic after 72 hours, on stainless steel after 48 hours and for less than 24 hours on cardboard and less than 4 hours on copper (4). Individuals come into contact with the pathogen at which point the virus can colonise the respiratory system. The time from first contact with the virus and the individual displaying symptoms is known as the incubation period. There is a significant range in the incubation period for COVID-19 in academic literature: 2-14 days. (5)
Our best estimates suggest that the R0 value, or basic reproductive number for COVID-19 is between 2.24-3.58 (5). This signifies that each infected individual will infect approximately three other susceptible individuals who will display symptoms. Below is a list of epidemics and their associated Ro values.
Median Ro Value
- SARS-CoV 2= 2.79 (6)
- 2009 seasonal influenza= 1.48 (7)
- 1918 pandemic influenza= 1.8 (7, 8)
At first, the difference between SARS-CoV 2, the virus behind the COVID-19 pandemic, and other listed respiratory viruses seems negligible. However ten iterations out, only ten generations of infected individuals, shows the significance of the SARS-CoV 2 high basic reproductive number. The number of cases of each infection at 10 generations can be calculated by 10 to the power of the basic reproductive number (Ro).
10 generations of infected individuals causes:
- SARS-CoV 2= 28578 cases
- 2009 seasonal influenza= 50 cases
- 1918 pandemic influenza= 357 cases
Now we can see the huge significance of the high basic reproductive number of SARS-CoV 2 and thus the significance of breaking the chain of infection.
Over the next few days we shall continue our examination of current medical literature on the COVID-19 pandemic. We shall cover the clinical characteristics of the virus, including: susceptible groups, symptoms, signs and measures to slow the spread. Then we shall touch on the moral and ethical challenges presented by the virus.
Until then, stay safe.
References
https://www.nejm.org/doi/full/10.1056/NEJMp2004361 (1)
https://www.sciencedaily.com/releases/2020/03/200317175442.htm (2)
https://www.who.int/gho/road_safety/mortality/traffic_deaths_number/en/ (3)
https://www.nejm.org/doi/full/10.1056/NEJMc2004973?query=featured_home (4)
https://www.sciencedirect.com/science/article/pii/S1201971220300539 (5)
https://academic.oup.com/jtm/article/27/2/taaa021/5735319 (6)
https://bmcinfectdis.biomedcentral.com/articles/10.1186/1471-2334-14-480 (7)
https://www.nature.com/articles/nature03063?page=21 (8)
P.S. if you have got this far my sincere thanks for reading. Please let me know any comments or feedback that you may have. I am very interested in engaging with those reading this blog including those who live outside the UK who will have alternative perspectives.
