

Wednesday 25th March 2020
One (Silly) Doc’s Story
The day started at 0630 with my alarm jarring me awake. I hit the snooze button for a further ten minutes rest before eventually resigning my fate to get up for work with the second alarm. A run through my morning routine in autopilot before dashing for the 0715 bus to work. I sip my protein shake breakfast as I observe the empty streets. The bus is all but empty, except for a few hospital workers that I recognise from the morning commute.
I arrive at work in record time given the lack of traffic and stops required by passengers on the journey. I head inside to the hospital. As I ascend the stairs to the office an idea to check the work rota arises. I don’t know why or how, but it does. I ponder this thought as I enter the ward. I open the rota on my phone as I walk through the doors of the doctor’s office. Wednesday 25th March- Annual Leave. Shit.
I say hello to my colleagues and double check that it is indeed Wednesday and it is the 25th March. To my dismay it is. I resign to my fate that I have come into work on my day off. I explain the situation to my colleagues who have a laugh and then proceed to tell me to go home. I get a situation report on the state of ward affairs. It appears we have all but become a respiratory ward, caring for respiratory boarders. We even have a respiratory consultant and middle grade doctor lead a ward round. This is of course in addition to our normal cardiac and thoracic ward rounds. I’m looking forward to that one tomorrow…
Examining COVID-19
We shall continue our examination of some interesting medical literature surrounding COVID-19 today.
Today global cases of COVID-19 passed 450,000 and deaths sadly passed 20,000. The number of cases is likely a gross underrepresentation of the true prevalence given that many countries are not testing cases in the “community”, or outside of hospitals and doctor’s surgeries. As such, many individuals with mild cases of COVID-19 will be conservatively managed at home with simple remedies and will never show up on the statistics. What does a case of COVID-19 look like though?
How does COVID-19 present?
For the majority of individuals COVID-19 will present with features associated with upper respiratory tract infection: dry cough, fever, shortness of breath, malaise or tiredness and altered smell and/or taste. Fever was the most common symptoms (92.8% cases), followed up cough (69.8% cases) and shortness of breath (34.5% cases). Notably a runny nose and sore throat were infrequently seen (<5% cases).
In a limited, small study males (61.7% cases) were more commonly affected than women. Patients requiring hospital admission and admission to intensive care typically had co-existing medical conditions or “co-morbidities”. Cardiovascular disease, diabetes and hypertension were most common co-morbidity seen in patient severely affected by COVID-19 infection. (1) It is worth noting that there is no proven causal link between these conditions and poorer outcomes from COVID-19. The effect on these particular co-morbidities on disease course from COVID-19 is yet to be fully determined.
However, one study has theorised that patients with diabetes and hypertension, who are often treated with ACE-inhibitors (an antihypertensive medication), express higher levels of an enzyme called ACE-2. Human coronaviruses bind to the ACE-2 enzyme. Therefore this study hypothesises that individuals such as diabetics and those treated with ACE-inhibitors are more susceptible to severe and fatal disease from COVID-19. (2)
Should I be worried?
Both adults and children have been noted amongst affected cases of COVID-19. However the WHO evidence suggests that those over the age of 60 years are prone to more severe infection. This fact has not been missed by governments. (3) The UK government recently announced that all individuals over the age of 70 must self-isolate for the next 12 weeks.
Children, who have accounted for up to 5% of cases so far globally, present with milder cases of infection. Infection in children presents with the same symptoms as adults. Fortunately mortality in children due to COVID-19 is extremely rare. (4) However it is far from Elon Musk’s comments on social media that children are essentially immune from the infection. This was an irresponsible and potentially damaging comment from the Space-X and Tesla boss. This highlights the potential for misinformation to be distributed in the age of instant publication via Facebook, Twitter and (ironically) blogs.
What does COVID-19 look like?
COVID-19 presents with atypical pneumonia, classically with both lungs involved and specific radiological changes. On chest x-rays a pattern of fluffy, white opacification and areas of ‘consolidation’, which indicates potential areas of infection, is seen. Eventually patients develop ‘ground glass changes’, which are regions of hazy lung opacification.

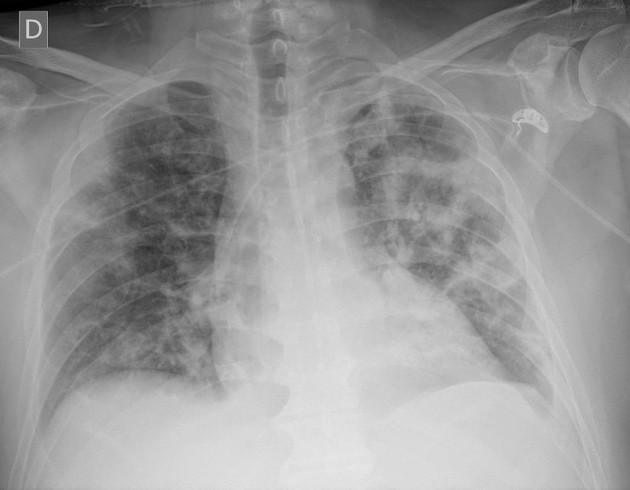
A chest x-ray of a patient with COVID-19. Note fluffy, white patches in both lung field which is typical of severe COVID infection. Case courtesy of Dr Edgar Lorente, Radiopaedia.org. From the case rID: 75264
Mild to moderate infections will require supplementary oxygen therapy and other supportive therapies. There is currently no definitive anti-viral treatment regime effective for COVID-19. But the scientific community is rapidly searching for this answer.
Severe infections can eventually develop an acute lung injury, known as acute respiratory distress syndrome (ARDS). This occurs when damage to the lung causes fluid to leak into the oxygen-exchange areas of the lung. As you can imagine, this fluid stops the effective exchange of oxygen into the body and carbon dioxide out of the body. As such, oxygen concentrations in the body fall and CO2 builds up. This leads to increased respiratory efforts as infected individuals work harder to move air into and out of their lungs, eventually leading to exhaustion. ARDS is associated with high rates of mortality; up to 50% ARDS patients die. (5) One study showed around 20% of COVID-19 patients who are admitted to hospital will develop ARDS and up to 8% will require mechanical ventilation.
What’s all the fuss about ventilation?
First we should outline the term ventilation. Ventilation within houses and buildings can be defined as the provision of fresh air into a space. This concept remains true in the lungs. Medical ventilation provides an artificial means of moving air into and out of the body when a patient becomes too unwell or exhausted to do this themselves. There have been calls from governments to rapidly increase the rate of ventilators produced and many companies have diverted their production lines to produce this piece of life saving medical equipment.
Well, that was a long read and pretty heavy stuff. If you’ve made it this far let’s end today’s blog entry on an upbeat note about compassion. Today 405,000 people have volunteered within the past 24 hours to aid the NHS in some form. 11,000 former medics and 24,000 final year nurses and medical students have answered the government’s rally cry. What a response. United we stand, divided we fall.
In other news…
References
(1) https://www.sciencedirect.com/science/article/pii/S0924857920300674
(4) https://onlinelibrary.wiley.com/doi/10.1111/apa.15270
(5) https://radiopaedia.org/articles/acute-respiratory-distress-syndrome-1?lang=us
